Blog

Minnesota Medicaid providers face a new EVV (Electronic Visit Verification) enforcement schedule in 2026.
Beginning January 1, 2026, agencies must submit EVV records for all in-home personal care and home health visits and achieve 50% verified visits to meet Minnesota EVV compliance requirements.
By July 1, 2026, the bar rises to 80%. DHS will issue corrective-action notices and may withhold or claw back payments for noncompliance.
– Minnesota Department of Human Services
This article explains the phased timeline and compliance rules, the data requirements and penalties & how large home care agencies should adjust operations – from scheduling, payroll, and billing to IT integration and training – to meet the mandate.
Minnesota DHS will phase in EVV compliance enforcement in 2026. Per DHS policy, effective Jan. 1, 2026, providers must enroll with the EVV aggregator and “submit complete data for all visits”.
They must meet 50% compliance for visits billed on/after that date. This initial phase is introductory – DHS will review Oct–Dec 2025 data & contact providers below 50% to raise awareness. In April 2026, DHS will formally audit Jan–Mar data and issue corrective-action letters to any provider still below 50%.
By July 1, 2026, the standard jumps: providers must achieve 80% EVV compliance on all billed visits. DHS will review Apr–Jun 2026 data and (initially) continue focusing enforcement on the 50% threshold, but notes that beginning October 2026 it will also issue notices to providers below 80%.
In practice, DHS will run quarterly compliance reports and escalate enforcement for noncompliance (requiring written improvement plans, meetings, and possibly payment stops or repayments).
Affected services: By state law and DHS policy, EVV in Minnesota covers all Medicaid-funded personal care and home health services requiring an in-home visit. In plain terms, that means any home or community-based service where the client receives help with ADLs or IADLs (e.g. PCA, home health aide, skilled nursing visits, therapies, supported living services, etc.).
Providers should refer to DHS’s detailed service code list for EVV to identify all in-scope services (e.g. PCA, AC, home health, waiver services).
Each EVV visit must capture the six federally-mandated points of data:
These data points must be transmitted to the EVV aggregator regardless of which Minnesota EVV software the agency uses.
Agencies must submit all visits (even if noncompliant or incomplete) into the EVV system. DHS emphasizes that missed/manually-entered visits count as noncompliance.
Every provider of EVV-eligible services – including private home care agencies and MCO-contracted providers – must enroll with the state aggregator data portal and submit EVV data.
DHS measures compliance at the agency level, combining data from all associated provider IDs. In practice, an agency’s overall compliance is the average of all sub-entity rates.
This means that even if one location or program is above 80%, another with low compliance can drag down the overall EVV compliance rate. Agencies are therefore responsible for all their NPIs meeting the threshold.
Under Minn. Stat. §256B.064 & DHS policy, failure to meet EVV requirements can trigger financial sanctions. DHS may issue corrective-action letters requiring a compliance improvement plan; if ignored, DHS can withhold or recoup payments for EVV services.
In extreme cases, payments may be stopped until EVV compliance is restored. Beyond state penalties, noncompliance risks federal funding cuts. The 21st Century Cures Act ties EVV to Medicaid FMAP funds, and many experts note that EVV creates an “auditable digital record” that deters fraud by proving services were delivered as billed.
In other words, insufficient EVV data could invite federal or state audits and force providers to return improperly paid Medicaid funds.
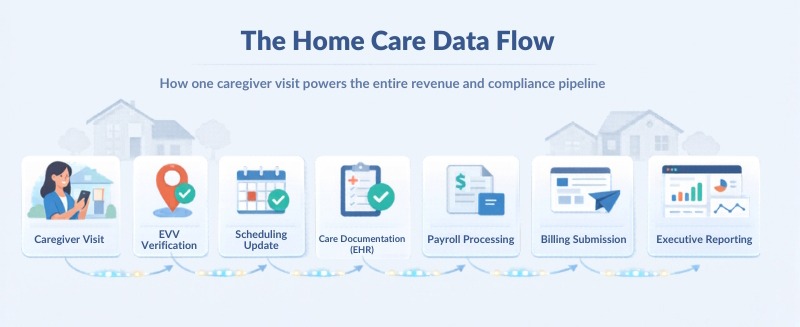
Implementing EVV affects nearly every aspect of agency operations. Key impacts include:
EVV systems usually require visits to be scheduled in advance. While this adds structure, it can improve efficiency. Experts report that EVV adoption often leads to better scheduling & coordination: it helps ensure staff coverage and reduces double booking.
Agencies may need to revise scheduling workflows or use scheduling modules within the EVV platform. Many agencies adopt Minnesota home care software with EVV that combines scheduling and verification in a single system.
EVV replaces paper timesheets with digital check-in/out. This can automate payroll: clock-in timestamps feed directly into pay calculations. Integrated EVV platforms often include payroll reporting & may link to time & attendance systems. The result is more accurate pay based on actual hours. Agencies must, however, adapt policies (e.g., OT rules) to align with electronic time stamps.
Integrated EVV software for Minnesota Medicaid providers can automatically feed visit timestamps into payroll systems, improving pay accuracy and reducing manual calculations.
EVV data validates billed units. DHS now allows providers to bill through the EVV system: the state aggregator can automatically submit compliant claims to DHS when all visit data & authorizations align.
In practice, linking EVV to billing ensures only verified visits are billed & can reduce claim denials.
EVV is distinct from clinical notes, but overlap exists. For example, an EVV visit record may include tasks performed. Agencies should integrate EVV with electronic health record (EHR) or care plan systems where possible, to avoid duplicate data entry.
Agencies need to connect multiple IT systems. At a minimum, the EVV vendor or state portal must integrate with DHS’s state aggregator. Ideally, EVV software for Medicaid programs should integrate with scheduling, EHR, payroll, billing, and reporting tools.
The state aggregator advises choosing “vertical connectivity” – a unified platform that “connects all stakeholders” (caregivers, providers, plans) for full visibility.
Training requirements are heavy. Agencies must train all staff and caregivers on using the EVV app or IVR, as well as on new agency policies and workflows. DHS guidance explicitly lists caregiver training as a provider responsibility.
Caregiver Training may include in-person sessions, online tutorials or job aids. Industry leaders advise setting realistic expectations and offering ongoing support.
EVV adds a technology burden on caregivers. If poorly managed, this can worsen turnover. To mitigate this, involve caregivers early and select user-friendly tools.
A well-implemented EVV can actually improve caregiver satisfaction by reducing paperwork. On the other hand, addressing concerns – such as connectivity in rural areas, privacy, or device access – is critical.
States that succeed invest in support resources (help lines, online help) so caregivers aren’t left struggling with the technology.
Minnesota allows a hybrid EVV model: agencies may use the state-provided system (HHAeXchange) at no cost, or a qualified third-party system (for which the provider pays).
Third party systems must transmit all required data to the state aggregator. Either way, full connectivity to the state aggregator is mandatory. When evaluating vendors, consider:
| Evaluation Factor | What to Consider |
|---|---|
| State compliance | Ensure the EVV system meets Minnesota Department of Human Services technical requirements and integrates with the state EVV data aggregator.
Ask vendors to provide proof of state aggregator integration and certification. |
| Scope of functionality | A strong EVV solution should do more than simple clock-in/clock-out. Look for scheduling integration, authorization checks, billing synchronization, payroll support, and reporting capabilities. |
| Vertical connectivity | Choose systems that connect payers, providers, and clients in one ecosystem, enabling data to move seamlessly across agencies. |
| Usability | Evaluate caregiver apps or IVR systems for ease of use. Confirm compatibility across device types and availability of multilingual support. Staff portals should also be intuitive for schedulers and supervisors. |
| Support and training | Assess the vendor’s onboarding and support resources. Look for implementation assistance, helpdesk access, training templates, documentation, and user guides. |
| Price vs. value | Compare total cost of ownership – not just subscription price. Consider implementation fees, device costs, IVR minutes, mobile data usage, and ongoing maintenance. |
A successful rollout needs a structured plan. Key milestones might include:
Establish EVV project team (sponsor, project manager, IT lead, compliance officer, training coordinator). Define scope (which programs, NPIs), map existing workflows & estimate budget (software, devices, training).
Large agencies often conduct an RFP process to evaluate vendors offering home care software with EVV capabilities.
Key considerations include:
Set up the EVV platform; build interfaces with scheduling/EHR/payroll systems; migrate any necessary data (e.g. employee lists, client rosters). Configure visit authorizations. Pilot the system with a small user group to find issues.
Deliver comprehensive training to all caregivers & office staff. Distribute devices or enroll staff in the EVV app. Conduct user acceptance testing. Official “go-live” should be before Jan 1, 2026 so that the 50% compliance period begins smoothly.
Track compliance consistently in the state aggregator portal. Address any shortcomings (e.g., send reminders to low compliance units & retrain staff). Make sure the written corrective plans are ready to submit, if requested by DHS.
Define roles & responsibilities clearly: e.g., CFO (budget approval), CIO (infrastructure), COO (process changes), HR/Training (staff training), Compliance Officer (monitoring reports).
Set measurable KPIs for the project and ongoing operation: for example, “% of EVV visits compliant” by month (target ≥50% after Jan 1, ≥80% after July 1); “% of staff/caregivers trained”; system adoption rate (e.g. what fraction of visits use EVV vs. manually entered); reduction in billing errors. Track DHS communications (no corrective actions ideally).
Budgets will vary (range unspecified). Large agencies should plan for software licensing (unless using free state aggregator only), IT integration costs, devices (smartphones/tablets if issuing them), and staff time for training and implementation.
Even if the state EVV system is free, internal expenses (IT hours, project management) can be significant. Management should allocate contingency funds for overtime or contractors if needed.
Anticipate the hurdles and have backup plans:
Ensure a backup verification method. For example, if an app is not working, caregivers must be trained to use IVR (phone) clock-in as a fallback.
Similarly, if mobile service is spotty, plan for offline mode or a fixed device clock in. Have additional devices/data plans in place, if required.
Plan for regular data audits. For e.g., reconcile payroll records with EVV logs every week to catch mis-entries. Correct all errors to not fall behind any compliance thresholds.
Ensure a fast onboarding process for new hires so they complete EVV training as soon as possible. Consider “train-the-trainer” models so knowledge isn’t siloed.
Create an EVV helpdesk/hotline, as experts recommend. Provide quick-reference guides & short video tutorials that cover common issues. For example, a simple step-by-step video on how to clock in would be invaluable for the new caregivers.
Devise a well-documented process to manage exceptions (e.g., a caregiver’s phone is broken, a client’s GPS is inaccurate, etc.). DHS indicates providers might be asked to “describe how they will improve compliance”. Thus, having contingency procedures in writing (e.g., manual sign-in forms to be entered into EVV) can showcase proactive planning.
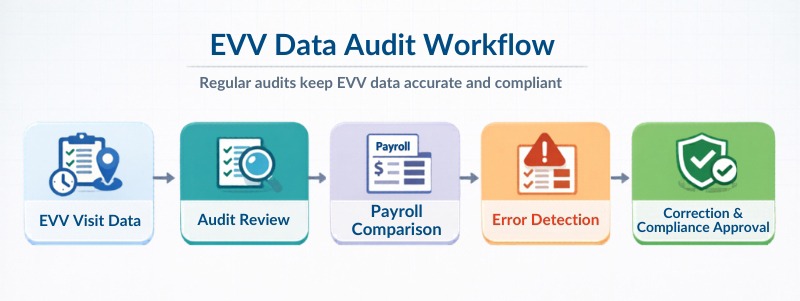
These policies demonstrate proactive compliance management & help agencies maintain strong EVV Minnesota compliance performance during audits.
Looking for EVV software built for Minnesota Medicaid compliance? See how CareSmartz360 helps agencies integrate EVV with scheduling, billing, payroll, and reporting.
Transparently address privacy in your communications. If using GPS, assure clients it only records coordinates at clock-in/out times. Minnesota guidance emphasizes aligning EVV with person-centered care – the technology should not be a barrier. For example, ensure that apps have simple interfaces & clear indications that EVV data is secure & only for billing purposes.
By planning for these scenarios, home care agencies can avoid compliance gaps.
Minnesota’s phased EVV enforcement in 2026 signals a shift from awareness to accountability. For large & growing home care agencies navigating Minnesota EVV requirements, this is an operational transformation.
Agencies that treat EVV as a strategic capability instead of a regulatory burden will be best positioned to thrive. With compliance thresholds rising up from 50% in January 2026 to 80% by July 2026, providers must ensure systems, staff training & workflows are aligned well before enforcement intensifies.
The agencies that succeed will be those that integrate EVV with scheduling, payroll, billing, and reporting – turning compliance data into operational intelligence. In a highly-regulated environment, preparation today protects both revenue & reputation tomorrow.
See how enterprise home care agencies are preparing for Minnesota EVV compliance.
Providers below these thresholds may receive corrective-action notices and increased monitoring.
For agencies operating in Minnesota:
By connecting EVV with operational systems, CareSmartz360 helps providers meet Minnesota EVV requirements while reducing administrative workload.
Download Blog

